Last reviewed: December 16, 2021
*** For up-to-date information about the Omicron variant’s impact on COVID-19 therapeutics, refer to our variant clinical data summary.
- Overview
- Corticosteroids
- Anti-Cytokine Monoclonal Antibodies
- Anti-Interleukin Antibodies (e.g., Tocilizumab)
- Anti-GM-CSF Antibodies
- JAK Inhibitors
- Resources
- Multimedia
The following is a curated review of key information and literature about this topic. It is not comprehensive of all data related to this subject.
Overview
An important branch of therapeutics for COVID-19 involves approaches to limit or constrain an over-robust inflammatory immune response to the virus, which can often be fatal. Several categories of immunomodulators have been studied, from the least specific (corticosteroids targeting multiple different domains of immunity) to the most specific (a monoclonal antibody targeting a single epitope of the SARS-CoV-2 spike protein). This page covers many different types of immunomodulators studied for use in COVID-19 treatment.
Corticosteroids
Dexamethasone, a corticosteroid, has been found to have a mortality benefit in SARS-CoV-2 infection in a large (N=6,425) controlled trial (RECOVERY Collaborative Group, February 2021) and a WHO meta-analysis (N=1,705 patients) looking at the association between systemic corticosteroids and mortality in seven randomized clinical trials of critically ill patients with COVID-19. Likewise, several other forms of corticosteroids have shown some degree of clinical benefit in COVID-19 (Edalatifard, December 2020). In some patients who progress to severe COVID-19 disease, it appears that the host immune response may lead to lung injury and multisystem organ dysfunction (Huang, January 2020; Moore, May 2020). Multiple studies on the use of corticosteroids in severe COVID-19 are underway to determine how they may mitigate pathology resulting from hyperinflammation.
Corticosteroids have been studied via many routes of dosing, most commonly intravenous, but more recently the inhaled route, with studies of inhaled budesonide that have shown reduction in hospitalization among patients on inhaled budesonide as compared to usual care (Ramakrishnan, July 2021).
The hypothesized mechanism of action is multidimensional:
- Steroids downregulate the expression in airway epithelium of the ACE-2 receptor, the receptor that SARS-CoV-2 virus uses to gain entry into the body.
- There is a dampening effect of steroids on SARS-CoV-2 replication in vitro.
- Steroids may reduce a dysregulated hyperinflammatory airway immune response, thus decreasing damage from the inflammatory cascade (Agusti, April 2021).
Recently, emerging data have pointed to a possible differential benefit of corticosteroids among different subpopulations of hospitalized patients with COVID-19. The most salient factor seems to be age, with one secondary analysis of the international nonrandomized observational prospective COVIP study (N=3,082) showing a higher 30-day mortality in elderly (>70 years) critically ill patients with COVID-19 who were given corticosteroids as compared to those who were not treated with steroids (53% and 42%, respectively; p<0.001) (Jung, June 2021). This association held true after multiple adjustments (aOR for mortality with corticosteroids, 1.60 [95% CI, 1.26-2.04; p<0.001]). Notably, the original RECOVERY trial showed no effect of corticosteroids among the subpopulation aged >70 years.
Guidelines
IDSA guidelines recommend the use of dexamethasone (or equivalent dose of an alternative glucocorticoid) in SARS-CoV-2 infection among hospitalized patients with severe COVID-19 (defined as patients with SpO2 ≤94% on room air, or those who require either supplemental oxygen, mechanical ventilation or extracorporeal mechanical oxygenation) or those critically ill (defined as patients on mechanical ventilation and ECMO). Critical illness includes end-organ dysfunction as is seen in sepsis/septic shock. In COVID-19, the most commonly reported form of end-organ dysfunction is acute respiratory distress syndrome. IDSA does not recommend the use of corticosteroids among hospitalized patients with nonsevere COVID-19 (SpO2 >94%, not requiring supplemental oxygen).
NIH guidelines recommend dexamethasone in addition to remdesivir (unless remdesivir is not available) in patients hospitalized with nonsevere COVID-19 who require supplemental oxygen.
Dosing
- Dexamethasone 6 mg IV or PO for 10 days (or until discharge if earlier).
- Equivalent total daily doses of alternative oral glucocorticoids to dexamethasone 6 mg daily are methylprednisolone 32 mg and prednisone 40 mg.
- Methylprednisolone intravenously 2 mg/kg daily; dose tapered after 5 days; total dosing, 10 days).
- Budesonide 800 mcg inhaled BID for duration of symptoms.
Key Literature
In summary: To date, multiple randomized controlled trials have assessed the use of corticosteroids in hospitalized patients with COVID-19; overall, these studies suggest the use of dexamethasone or hydrocortisone reduces mortality in hospitalized patients with COVID-19 who require supplemental oxygen due to hypoxia (SpO2 ≤94% on room air) (RECOVERY Collaborative Group, February 2021). A number of observational studies have also been completed, and these have had mixed results; however, randomized controlled trial data is most reliable. A few small studies have suggested that intravenous methylprednisolone (which is known to achieve higher lung concentrations than does dexamethasone) may be superior to dexamethasone in shortening hospital stay and time to clinical recovery in patients with severe COVID-19, with a trend toward lower mortality (Ranjbar, April 2021; Braude, October 1983).
Methylprednisolone or Dexamethasone, Which One Is Superior Corticosteroid in the Treatment of Hospitalized COVID-19 Patients (Ranjbar, April 2021).
Patient population:
- 86 adults hospitalized with hypoxia from confirmed SARS-CoV-2 infection were randomized to receive either IV methylprednisolone (2 mg/kg daily dose tapered after 5 days; total dosing, 10 days) or IV dexamethasone (6 mg daily for 10 days).
- Study took place at a single center in Shiraz, Iran, between August and November 2020.
- Participants were 61.4% and 52.4% male, and mean (SD) age was 56.2 (17.5) and 61.3 (17.3) in the methylprednisolone and dexamethasone groups, respectively.
Primary endpoint:
- All-cause mortality in 28 days.
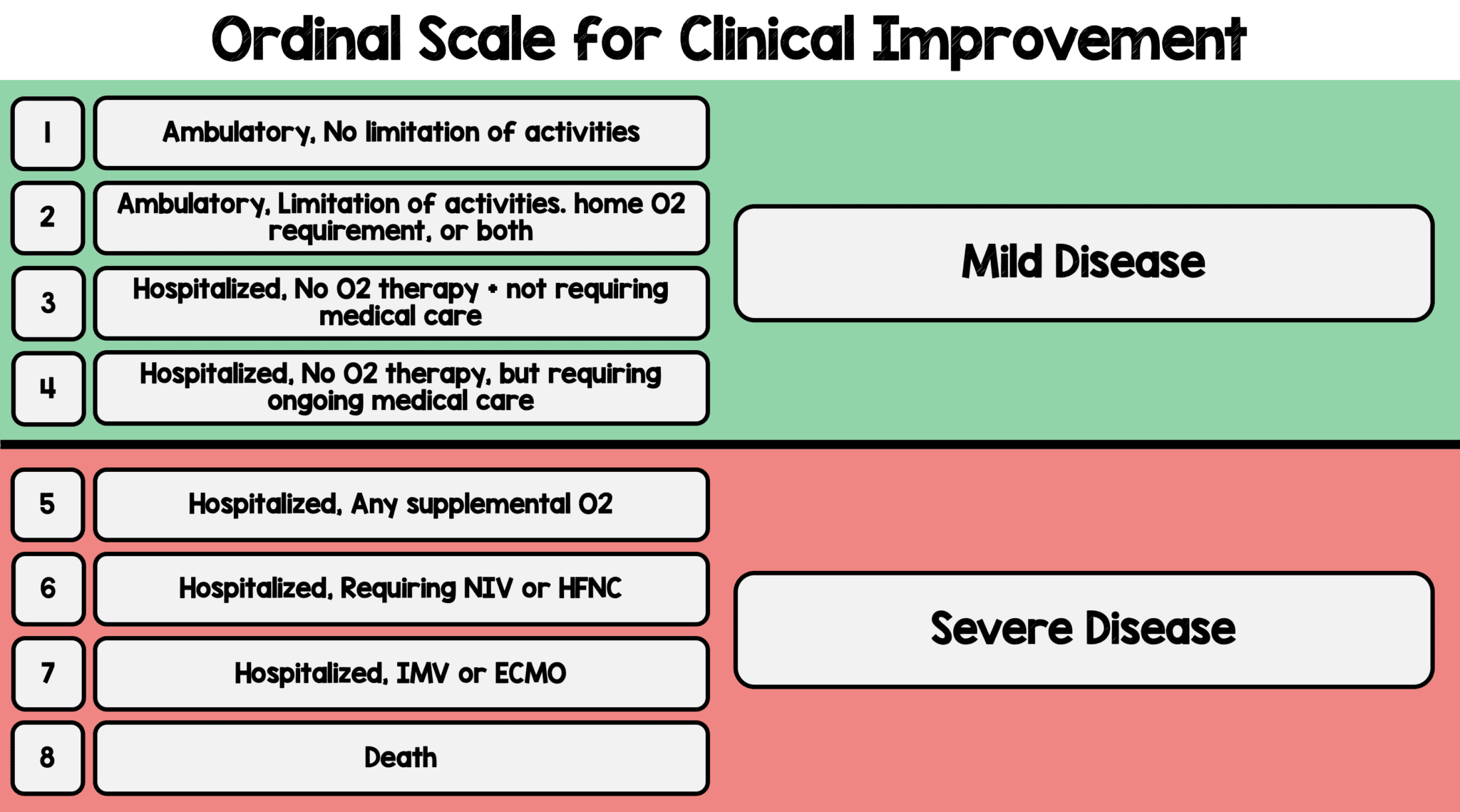
- Clinical status on 9-point WHO ordinal scale, at day 5 and day 10 from enrollment.
- Secondary endpoints included need for ICU admission or mechanical ventilation; exploratory endpoints were hospital length of stay and death within 28 days of enrollment.
Key findings:
- Patients assigned to receive methylprednisolone had better clinical improvement (measured using the 9-point WHO Ordinal Scale for Clinical Improvement, with 0 being uninfected and 8 being death) than patients who received dexamethasone.
- Day 5 OSCI score (4.02 methylpred vs. 5.21 dexamethasone, p=0.002).
- Day 10 OSCI score (2.90 methylpred vs. 4.71 dexamethasone, p=0.001).
- Overall mean OSCI score lower in methylprednisolone group than in dexamethasone group (3.909 vs. 4.873 respectively, p=0.004).
- Methylprednisolone patients also had significantly lower ventilator requirements (18% vs. 38%, with a number needed to treat of 5).
- Methylprednisolone group had shorter hospital length of stay: mean length of stay was 7.43 ± 3.64 and 10.52 ± 5.47 days in the methylprednisolone and control groups, respectively (p=0.015).
- Methylprednisolone group had a trend toward lower mortality (19% vs. 38%; NNT, 6; p=0.076), compared with dexamethasone patients.
{kind=link}
Limitations:
- Small size, single center, racially/ethnically homogeneous.
- Limited information on clinical features such as CT chest findings.
Comparison of Efficacy of Dexamethasone and Methylprednisolone in Moderate to Severe COVID-19 Disease (Fatima, December 2020).
Overall, in this quasi-experimental study of 100 patients with COVID-19, there was an association of similar outcomes of dexamethasone and methylprednisolone in treating moderate to severe COVID-19 infection.
Patient population:
- Quasi-experimental, interventional study of 100 COVID-19 patients in Pakistan.
- 35 patients received dexamethasone, and 65 received methylprednisolone.
- Patients were also given tocilizumab and convalescent plasma as indicated.
- The mean age of patients was 57.91 years in the dexamethasone group and 54.86 years in the methylprednisolone group.
Primary endpoint:
- To compare the efficacy and safety of dexamethasone versus methylprednisolone in moderate to severe COVID-19.
Key findings:
- In the dexamethasone group, 15 critically ill patients (42.8%) were shifted to the ICU, and seven of them (20%) needed ventilator support.
- In the methylprednisolone group, 22 patients (33.8%) were admitted to the ICU with eight of them (12.3%) requiring ventilator support.
- Patients in both groups showed marked improvement in temperature, oxygen requirement and C-reactive protein on day 5.
- Six patients who received dexamethasone died (17.1%) versus 10 patients (15.3%) who received methylprednisolone.
Limitations:
- Small sample size and single-center study, which may limit generalizability of results.
- A higher percentage of patients in the dexamethasone group were critically ill and required ventilator support.
- Patients also received antibiotics, tocilizumab and convalescent plasma, which may have impacted results.
- Median time from start of corticosteroids upon admission to hospital was not stated.
Corticosteroid Therapy for Coronavirus Disease 2019-Related Acute Respiratory Distress Syndrome: A Cohort Study With Propensity Score Analysis (Wu, November 2020).
Overall, in this single-center retrospective study of 382 patients, low-dose corticosteroid treatment was associated with reduced risk of in-hospital death within 60 days in COVID-19 patients who developed acute respiratory distress syndrome.
Patient population:
- Single-center retrospective observational study of 382 patients with acute respiratory distress syndrome caused by COVID-19 between Jan. 20 and Feb. 24, 2020.
- 226 patients (59.2%) received systemic corticosteroids, and 156 (40.8%) received standard treatment.
- Among patients prescribed corticosteroids, methylprednisolone was the most frequently administered (213/226, 94.2%).
- The maximum dose of corticosteroids was 80.0 (IQR, 40.0-80.0) mg equivalent methylprednisolone per day, and duration of corticosteroid treatment was 7.0 (4.0-12.0) days in total.
- Overall, the mean age ± SD was 60.7 years ± 14.1.
- The median was 2.0 (IQR, 2.0-3.0). Of these cases, 94 (24.6%) patients had invasive mechanical ventilation.
- Corticosteroids were more likely to be prescribed to younger (p=0.0077) and male (p=0.0135) patients.
Primary endpoint:
- To compare the risk of 60-day in-hospital mortality between COVID-19-related acute respiratory distress syndrome patients with corticosteroid treatment and those without.
Key findings:
- The 60-day hospital death rate in patients who ever used corticosteroids was higher than the patients who did not use corticosteroids (135 [59.7%] vs. 68 [43.6%], p=0.0019).
- The median survival duration was longer in the corticosteroid group (19.0 [IQR, 15.0–21.0] vs. 15.0 [IQR, 12.0-23.0], p=0.0239).
- In Cox regression analysis using corticosteroid treatment as a time-varying variable, corticosteroid treatment was associated with a significant reduction in risk of in-hospital death within 60 days after adjusting for age, sex, SOFA score at hospital admission, propensity score of corticosteroid treatment, comorbidities, antiviral treatment and respiratory supports (HR, 0.42; 95% CI, 0.21-0.85; p=0.0160).
- In the Cox regression model, there was no difference in time to viral shedding between the corticosteroids-treated group and the standard of care group (HR, 1.43; 95% CI, 0.43-4.80; p=0.5593).
Limitations:
- This was not a randomized controlled trial; selection bias and the potential of confounding effects may exist.
- Only measured factors were controlled for due to the nature of observational study design.
- This study was single center in design; therefore, there may be lack of generality.
Corticosteroid Treatment in Severe COVID-19 Patients With Acute Respiratory Distress Syndrome (Liu, November 2020).
Overall, in this multicenter retrospective study, administration of corticosteroids, primarily methylprednisolone, in severe COVID-19-related acute respiratory distress syndrome was associated with increased 28-day mortality and delayed SARS-CoV-2 coronavirus RNA clearance after adjustment for time-varying confounders.
Patient population:
- Retrospective multicenter study of 774 patients with COVID-19 and acute respiratory distress syndrome.
- 409 patients received corticosteroids, with a median time from hospitalization to starting corticosteroids of 1.0 day (IQR, 0.0-3.0 days); 365 patients received standard of care.
- Methylprednisolone was the most frequently used corticosteroid (396 of 409 [96.8%] patients) followed by prednisolone (32 of 409 [7.8%] patients). The maximum daily hydrocortisone-equivalent median dose of 200 mg (IQR, 200-400 mg) was used. The median duration of corticosteroid therapy was 6.0 days (IQR, 4.0-10.0 days).
- The median age was 64 years (IQR, 54-73 years), and 452 (58.0%) were male.
- 596 patients (77%) had one or more comorbidities.
- The median was 11 (IQR, 9-13).
Primary endpoint:
- To explore the effects of corticosteroids on mortality from COVID-19 with acute respiratory distress syndrome and on the clearance of SARS-CoV-2 RNA compared to those receiving standard of care.
Key findings:
- At 28 days, 181 of 409 (44.3%) patients in the corticosteroid group had died and 113 of 365 (31.0%) in the control group (OR, 1.77; 95% CI, 1.32-2.38; p<0.001).
- 185 out of 409 (45.2%) corticosteroid-treated patients died during hospitalization, compared with 115 of 365 (31.5%) controls (OR, 1.79; 95% CI, 1.34-2.41; p<0.001).
- Multivariate logistic regression analysis suggested increased 28-day mortality with corticosteroids (adjusted OR, 2.17; 95% CI, 1.36-3.53; p=0.001).
- After applying propensity score matching, 182 control and 182 case patients were matched. Corticosteroid therapy was significantly associated with increased 28-day mortality in multiple analyses, including Kaplan-Meier survival plot, multivariable logistic regression model (adjusted OR, 1.64; 95% CI, 1.05-2.57; p=0.032) and extended multivariable Cox regression model, which treated corticosteroid use as a time-varying exposure variable (adjusted HR, 1.46; 95% CI, 1.01-2.13; p=0.045).
- In subgroup analyses, high dose (>200 mg) and early initiation (≤3 days from hospitalization) of corticosteroid therapy were associated with a higher 28-day mortality rate.
- Corticosteroid therapy was associated with delayed SARS-CoV-2 RNA clearance among survivors by log-rank test (p=0.00017).
Limitations:
- Retrospective design and some heterogeneity in the population, partly related to critically ill patients treated outside the ICU due to shortages in ICU beds.
- Some laboratory parameters (such as LDH, ferritin and CRP) were missing for some patients on admission, which may have introduced some biases.
- There was no long-term follow-up.
Intravenous Methylprednisolone Pulse as a Treatment for Hospitalized Severe COVID-19 Patients: Results From a Randomized Controlled Clinical Trial (Edalatifard, September 2020).
Overall, in this small single-blind randomized study, patients with severe COVID-19 receiving methylprednisolone pulse had a significantly increased survival time, more clinical improvement and lower mortality compared to those receiving standard of care.
Study population:
- A single-blind, randomized, controlled, clinical trial of 68 hospitalized patients with confirmed severe COVID-19 in Iran.
- Included patients were nonintubated adults, had confirmed COVID-19, SpO2 <90%, CRP >10 and IL-6 levels of >6.
- 34 patients were assigned to receive standard care and pulse-dose methylprednisolone (250 mg/day for 3 days) and 34 patients to standard care alone.
- The mean age of patients was 58.5±16.6 years old; 62.9% were men.
Primary endpoint:
- Time of clinical improvement or death, whichever came first.
Key findings:
- 22 patients (35.5%) had respiratory rate >24 breaths/min, and 13 patients (21.0%) had heart rate >100 beats/min.
- The median interval time between disease symptom onset and hospitalization was 6.8±2.97 days.
- Patients with clinical improvement were higher in the methylprednisolone group compared to the standard-of-care group (94.1% vs. 57.1%), and the mortality rate was numerically lower in the methylprednisolone group (5.9% vs. 42.9%; p<0.001).
- Patients in the methylprednisolone intervention group had a significantly increased survival time compared with the patients in the standard of care group (log rank test: p<0.001; HR, 0.293; 95% CI, 0.154-0.556).
- Six patients in the SOC group received corticosteroids from their prescribing physician and were excluded from the analysis.
Limitations
- Single-blind design.
- Six of the 34 patients (approximately 18%) in the SOC group were excluded from the analysis due to receiving corticosteroids; this could have altered the results, particularly given the small sample size.
- Lack of patient follow-up to identify long-term adverse events.
Association Between Administration of Systemic Corticosteroids and Mortality Among Critically Ill Patients With COVID-19: A Meta-Analysis (WHO REACT Working Group, September 2020).
Overall, in this prospective meta-analysis of seven randomized trials consisting of 1,703 patients, 28-day all-cause mortality was lower among patients who received corticosteroids compared with those who received usual care or placebo. While a little over half of the weight of the study was due to the RECOVERY trial, findings were consistent across studies. This meta-analysis further supports the use of corticosteroids in critically ill patients with COVID-19 who require respiratory support.
Study population:
- Meta-analysis of seven randomized controlled trials from 12 countries, consisting of 1,703 critically ill patients with COVID-19.
- Patients were randomized to receive systemic dexamethasone, hydrocortisone or methylprednisolone (678 patients) or standard of care/placebo (1,025 patients).
- Median age was 60 (IQR, 52-68), and 29% were female.
Primary endpoint:
- To estimate the association between administration of corticosteroids compared with usual care or placebo and 28-day all-cause mortality.
Key findings:
- Seven trials were included; six trials were assessed as “low concern” for bias; one was assessed as “some concerns.”
- The I2 was 15.6% (p=0.31), indicating little heterogeneity between the trials.
- There were 222 deaths among the 678 patients randomized to corticosteroids, and 425 deaths among the 1,025 patients randomized to usual care or placebo (summary OR, 0.66 [95% CI, 0.53-0.82]) based on a fixed-effect meta-analysis.
- The absolute mortality risk of 32% with corticosteroids compared with an assumed mortality risk of 40% with usual care or placebo.
- The association between administration of corticosteroids and reduced mortality was similar for dexamethasone and hydrocortisone.
- Among the six trials that reported serious adverse events, 64 events occurred among 354 patients randomized to corticosteroids, and 80 events occurred among 342 patients randomized to usual care or placebo.
Limitations:
- Two of the seven trials reported mortality at 21 and 30 days, respectively; this may have led to inconsistencies in the results.
- Only adults were included in the trials, and most of them were conducted in high-income settings. This may limit the generalizability of the results.
- The majority of patients in the placebo/usual care arm were from the RECOVERY trial (59.1%), and overall, RECOVERY contributed 57% to the weight in the analysis; this may have skewed the results.
Effect of Systemic Glucocorticoids on Mortality or Mechanical Ventilation in Patients With COVID-19 (Keller, August 2020).
Overall, in this retrospective observational study, corticosteroid-treated patients with markedly elevated C-reactive protein benefited from corticosteroid treatment, while patients with lower CRP had higher mortality.
Study population:
- 1,806 patients admitted with COVID-19 in a New York City health system.
Primary endpoint:
- Mortality or need for mechanical ventilation.
Key findings:
- 140 patients (7.7%) were treated with corticosteroids, while 1,666 (92.3%) never received corticosteroids.
- Corticosteroid use in patients with initial CRP levels >20 mg/dL was correlated with significantly reduced risk of mortality or mechanical ventilation (OR, 0.23; 95% CI, 0.08-0.70).
- Corticosteroid use in patients with CRP levels <10 mg/dL was associated with significantly increased risk of mortality or mechanical ventilation (OR, 2.64; 95% CI, 1.39-5.03).
Limitations:
- Retrospective, single-center observational design; therefore, confounding factors cannot be excluded.
- The type, dose and route of corticosteroid use is not reported.
Methylprednisolone as Adjunctive Therapy for Patients Hospitalized With COVID-19 (Metcovid): A Randomized, Double-blind, Phase IIb, Placebo-controlled Trial (Jeronimo, August 2020).
Overall, in this randomized controlled trial, a short course of methylprednisolone in hospitalized patients with COVID-19 did not reduce mortality.
Study population:
- 416 hospitalized patients with confirmed or suspected COVID-19 disease at a single center in Brazil; infection was confirmed in 81.3% of patients.
- Patients received methylprednisolone (0.5 mg/kg twice daily for 5 days) or placebo.
- 393 patients were included in a modified intention-to-treat analysis.
Primary endpoint:
- 28-day mortality.
Key findings:
- 28-day mortality was 76/199 (38.2%) in the placebo group, versus 72/194 (37.1%) in the methylprednisolone group (p=0.629)
- Post-hoc analysis showed reduced mortality in the methylprednisolone group compared to the placebo group (52/84 or 61.9% vs. 34/73 or 46.65%; p=0.039).
Limitations:
- Single-center study.
- Authors used a modified intention-to-treat analysis; of 416 patients randomized, 393 were analyzed. While this could have affected the balance of the groups, the authors note similar findings with an intention-to-treat analysis.
Dexamethasone in Hospitalized Patients With COVID-19 (The RECOVERY Collaborative Group, July 2020).
Overall, in this controlled open-label trial, dexamethasone reduced mortality in those patients receiving mechanical ventilation or oxygen. There was no benefit for patients who did not require respiratory support; in fact, there was a non-statistically significant trend toward increased mortality.
Study population:
- 6,425 patients admitted with COVID-19 disease to 176 National Health Service hospitals in the U.K., of whom 2,104 were randomly allocated to receive dexamethasone (6 mg/day for up to 10 days) plus standard of care and 4,321 received standard of care alone.
Primary endpoint:
- All-cause mortality within 28 days of randomization.
Key findings:
- 482 patients (22.9%) in the dexamethasone arm and 1,110 patients (25.7%) in the standard of care group died within 28 days of randomization (p<0.001).
- In the dexamethasone group, the incidence of death was lower than the standard-of-care arm among patients receiving mechanical ventilation (29.3% vs. 41.4%; RR, 0.64; 95% CI, 0.51-0.81), as well as those receiving oxygen without mechanical ventilation (23.3% vs. 26.2%; RR, 0.82; 95% CI, 0.72-0.94)
- In patients who were moderately ill but did not require oxygen at baseline, use of dexamethasone was associated with a non-statistically significant finding of increased mortality (17.8% vs. 14.0%; RR, 1.19; 95% CI, 0.91-1.55).
Limitations:
- The mortality rate of patients with severe COVID-19 found in this study is higher than what has been generally found in this group in the United States.
- Open-label design; researchers and patients in the study knew who was receiving which treatment. This could have introduced bias into the results.
- Not all patients had proven SARS-CoV-2 infection via RT-PCR.
- There was variability in how long patients received dexamethasone (the range was 3-10 days).
Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With COVID-19 in Wuhan, China (Wu, July 2020).
Overall, in this retrospective cohort study, among patients with ARDS, treatment with methylprednisolone was associated with significantly better outcomes.
Study population:
- 201 hospitalized patients with COVID-19 at a single center in Wuhan, China.
Primary endpoint:
- Development of ARDS; death.
Key findings:
- 84 patients (41.8%) developed ARDS, of whom 44 (52.4%) died.
- Among patients with ARDS, of those who received methylprednisolone treatment, 23 of 50 (46%) died, while of those who did not receive methylprednisolone, 21 of 34 (61.8%) died.
- In bivariate Cox regression analysis, among patients with ARDS, treatment with methylprednisolone decreased the risk of death (HR, 0.38; 95% CI, 0.20-0.72).
Limitations:
- Single-center retrospective study; therefore, the presence of confounding factors cannot be excluded.
- At the time, only patients with severe disease were hospitalized.
- Only 10% of patients without ARDS were administered methylprednisolone; it is not disclosed if methylprednisolone was associated with lower death rate in the non-ARDS cohort.
- Symptom duration before methylprednisolone administration was not reported for any group.
Early Short-Course Corticosteroids in Hospitalized Patients With COVID-19 (Fadel, May 2020).
Overall, in this nonrandomized intervention study, an early short course of methylprednisolone in patients with moderate to severe COVID-19 reduced escalation of care and improved clinical outcomes. The results are limited by the use of other therapeutic agents.
Study population:
- 213 patients with moderate to severe COVID-19 who received either standard of care, or standard of care and methylprednisolone 0.5 to 1 mg/kg/day divided in two intravenous doses for 3 days.
- Standard of care included antibiotic agents, antiviral agents or tocilizumab, as determined by the primary team.
Primary endpoint:
- Composite endpoint of escalation of care from ward to ICU, new requirement for mechanical ventilation and mortality.
Key findings:
- 81 patients were included in the standard of care group and 132 in the early corticosteroid group.
- The composite endpoint happened at a lower rate in the early corticosteroid group (34.9% vs. 54.3%; p=0.005).
- A significant reduction in median hospital length of stay was seen in the early corticosteroid group (8 vs. 5 days; p<0.001).
- Multivariate regression analysis demonstrated an independent reduction in the composite endpoint at 14 days controlling for other factors (adjusted OR, 0.41; 95% CI, 0.22-0.77).
Limitations:
- Nonrandomized design; confounding factors cannot be excluded.
- Many patients with moderate-severe disease received lopinavir-ritonavir, ribavirin and hydroxychloroquine. Tocilizumab may also have been given. This could have affected results.
Additional Literature
Inhaled Therapies
As the SARS-CoV-2 virus enters the body through the respiratory route, the concentrations of antiviral in the airway epithelium can be considered most relevant for inhibiting initial viral replication in early infection. Delivering medications through a nebulized/inhaled route during early infection may avoid systemic toxicity.
STOIC Trial: Inhaled budesonide in the treatment of early COVID-19 illness (Ramakrishnan, February 2021 - preprint, not peer-reviewed). This Phase 2, randomized, controlled, open-label study assessed outcomes in nonhospitalized U.K. patients with mild COVID-19 who were randomized to receive either inhaled budesonide (800 µg dry powder inhaler twice daily) or placebo. Study participants were within 7 days of symptom onset, and those with recent use of systemic glucocorticoids were excluded. Endpoints included likelihood of requiring a COVID-19-related urgent care visit, emergency department care or hospitalization. Among 139 participants in the per-protocol analysis, the primary study outcome was reached in 1 of 70 participants in the budesonide arm and 10 of 69 participants in the standard of care arm (difference in proportion of 0.131, p=0.004; number needed to treat to prevent a single hospitalization was 8). Time to recovery was also reduced in the budesonide arm (median of 7 days versus 8 days in the usual care arm, log rank test p=0.007), and participants in the budesonide arm were less likely to have symptoms at day 14 (10% vs. 30% respectively, difference in proportion of 0.204, p=0.003). Of note, the study was not double blinded, and most participants were young and healthy, with low risk of progression to more severe disease; there was also no requirement that they have a positive SARS-CoV-2 test. (A sensitivity analysis among only participants with SARS-CoV-2 PCR-confirmed COVID showed a similar result: difference in proportion of 0.125, p=0.007.) The biological plausibility is twofold: 1) topical/inhaled steroids inhibit ACE-2 receptors, thus limiting viral entry; and 2) steroids may limit the airway inflammatory response to the virus. This is an encouraging proof-of-concept study among outpatients with mild COVID-19, and there is a need for larger-scale randomized controlled trials in multiple locales and with patients of older age and additional comorbidities.
Back to Top
Anti-Cytokine Monoclonal Antibodies
Early in the pandemic, there was a recognition that certain pro-inflammatory cytokines (including IL-6, CXCL-10 and GM-CSF) occur at much higher levels in COVID-19 patients with severe disease than with mild disease; similarly, levels were higher in patients who died from COVID-19 (Thwaites, March 2021; Henry, June 2020). In some patients who progress to severe COVID-19 disease, host immune response can lead to lung injury and multisystem organ dysfunction (Huang, January 2020; Moore, May 2020), and this has in part been attributed to the effects of cytokine cascades (Yang, February 2020; Mehta, March 2020).
Anti-Interleukin Antibodies
Antibodies against many specific interleukins are available, many with FDA approval for other indications. For example, tocilizumab is an IL-6 receptor monoclonal antibody that is approved for the use of CAR-T associated cytokine release syndrome. Due to similarities in the clinical presentation of CAR-T cytokine release syndrome and the hyperinflammatory state of severe COVID-19, interest in tocilizumab for severe COVID-19 developed early in the pandemic (Mehta, March 2020). Other agents that mitigate the effects of IL-6, including sarilumab and siltuximab, have also been investigated, although to a lesser extent. Lastly, anakinra, a monoclonal antibody that blocks the interleukin IL-1, has been studied for the treatment of COVID-19.
Although several observational studies have suggested mortality benefit from tocilizumab (Biran, August 2020; Somers, July 2020; Guaraldi, June 2020), data from randomized clinical trials of tocilizumab in COVID-19 did not show a benefit, and a meta-analysis of early studies found that there was no significant difference in 28-day mortality among tocilizumab-treated patients: pooled RR of death was 1.09 (95% CI, 0.80-1.49; I2=0%) (Tleyjeh, February 2021). The first randomized controlled trial information made publicly available was preliminary results of COVACTA, the Roche Phase 3 randomized controlled trial of tocilizumab among 452 patients hospitalized with severe COVID-19 pneumonia (Rosas, April 2021). The study, which randomized participants 2:1 to receive tocilizumab or placebo, found that there was no significant difference observed at day 28 between treatment groups in a seven-category ordinal scale rating clinical status. COVACTA also failed to meet its secondary endpoint of reduced patient mortality at week four. Sanofi/Regeneron’s sarilumab randomized controlled trial also indicated a failure to meet similar endpoints (unsurprisingly, as only 20% of participants were receiving systemic glucocorticoids in that study) (Lescure, May 2021). Some other peer-reviewed randomized trials have not shown a benefit of tocilizumab in 28-day mortality or clinical improvement in critically ill patients with COVID-19 (Salvarani, October 2020); limitations included small sample sizes and methodologic differences. One Phase 3 trial (REMDACTA) of 649 hospitalized patients with severe COVID-19 pneumonia has compared tocilizumab plus remdesivir to placebo plus remdesivir, to get at the question of whether tocilizumab has added efficacy when used alongside remdesivir. Its results showed no significant differences between treatment groups in the primary endpoint of time to hospital discharge or readiness for discharge at 28 days (Tleyjeh, February 2021).
In mid-June 2020, with the initial release of the results of the RECOVERY trial showing that the use of low-dose dexamethasone (6 mg) had a favorable impact on 28-day mortality among patients requiring oxygen for COVID (RECOVERY Collaborative Group, February 2021), there was a transition in the standard of COVID care, and patients began receiving dexamethasone as first-line therapy for COVID. After this point, once trial populations began including a majority of patients on concomitant corticosteroids, randomized controlled trial data on tocilizumab began to reinforce the benefit from tocilizumab seen in the early observational studies.
Preliminary results released via press release from Roche’s Phase 3 EMPACTA trial noted the study’s primary endpoint had been met: Hospitalized patients who received tocilizumab were 44% less likely to progress to mechanical ventilation or death compared with patients who received placebo plus standard of care (in the final publication, among 389 patients, the hazard ratio for the primary outcome of mechanical ventilation or death was 0.36 [95% CI, 0.33-0.97] in the tocilizumab group as compared to the placebo group) (Salama, January 2021). This was based on the finding that the primary outcome (mechanical ventilation or death) was met for 12% of patients receiving tocilizumab as compared to 19.3% of patients receiving placebo. Of note, 79% of the patients in EMPACTA were also receiving corticosteroids. Other small studies followed. The REMAP-CAP study of tocilizumab or sarilumab versus control also had 92% of participants on corticosteroids, and also showed increased survival with tocilizumab or sarilumab as compared to the control group (survival at 90 days HR, 1.61 [95% CI, 1.25-2.08].
These results were recapitulated in much larger trials, like the RECOVERY trial, which randomized 4,116 patients with severe COVID-19 pneumonia and CRP ≥75 mg/L to receive either tocilizumab plus usual care (2,022 patients) or usual care alone (2,094 patients) (RECOVERY Collaborative Group, May 2021). The primary endpoint of mortality by day 28 was reached in 30.7% of patients receiving tocilizumab as compared to 34.9% of patients receiving usual care alone (rate ratio, 0.85; 95% CI, 0.76-0.94; p=0.0028). Time to hospital discharge was also shortened in the tocilizumab group, with median time to hospital discharge of 19 days as compared to >28 days for patients in the usual care group. Eighty-two percent of participants in the RECOVERY trial were receiving systemic steroids. It is noteworthy that the mortality rate in both arms of this trial was so much higher than the mortality rate in the other tocilizumab trials, for reasons that remain unclear but may represent secular or regional trends in SARS-CoV-2 treatment practices.
Of high interest for the current pandemic, randomized controlled trials of tocilizumab versus standard of care done entirely in low- and middle-income countries are beginning to be reported. One recent study, the COVINTOC trial in India, found no added benefit of tocilizumab in preventing the progression/worsening of COVID at day 14, even in the setting of 91% of the participants being on corticosteroids (Soin, March 2021). Certain subsets of patients, however, such as patients with severe disease at baseline, did appear to derive benefit, which will be further explored in forthcoming trials.
Anti-IL-1β antibodies have also been studied for severe COVID. One randomized controlled trial examined the anti-IL-1β antibody canakinumab in 454 hospitalized patients with severe COVID-19 and elevated inflammatory markers not yet on mechanical ventilation (Caricchio, July 2021). There was no significant difference in mechanical ventilation-free survival between the two groups (88.8% in canakinumab and 85.7% in placebo groups).
Guidelines
IDSA guidelines conditionally suggest the use of tocilizumab in addition to standard of care (i.e., steroids) rather than standard of care alone among hospitalized patients with progressive severe or critical COVID-19.
- When tocilizumab is not available, IDSA guidelines suggest sarilumab in addition to standard of care (i.e., steroids) rather than standard of care alone.
NIH guidelines recommend using tocilizumab (single intravenous dose of tocilizumab 8 mg/kg actual body weight up to 800 mg) only in combination with dexamethasone (6 mg daily for up to 10 days or an alternative corticosteroid at a dose equivalency to dexamethasone 6 mg) in certain hospitalized patients who are exhibiting rapid respiratory decompensation due to COVID-19.
- NIH panel found that there are insufficient data to recommend either for or against the use of sarilumab for hospitalized patients with COVID-19 who are within 24 hours of admission to the ICU and who require invasive mechanical ventilation, noninvasive ventilation or high-flow oxygen.
- NIH panel recommends against the use of siltuximab for the treatment of COVID-19 except in a clinical trial.
- Tocilizumab should be avoided in “patients who are significantly immunosuppressed, particularly in those with recent use of other biologic immunomodulating drugs, and in patients who have alanine aminotransferase >5 times the upper limit of normal; high risk for gastrointestinal perforation; an uncontrolled serious bacterial, fungal or non-SARS-CoV-2 viral infection; absolute neutrophil count <500 cells/µL; platelet count <50,000 cells/µL; or known hypersensitivity to tocilizumab.”
- In patients given tocilizumab, prophylactic treatment with ivermectin should be considered for those who are from strongyloidiasis endemic areas.
FDA has issued an EUA for tocilizumab for use in hospitalized patients, ages 2 and up, with severe COVID-19. The intended population includes patients receiving corticosteroids and requiring some form of supplemental oxygen, mechanical ventilation or ECMO.
Key Literature
In summary: There is now a moderate body of evidence that tocilizumab, when used in conjunction with systemic corticosteroids such as dexamethasone to treat COVID-19 in hospitalized patients, does confer a mortality benefit. The trials showing the most benefit (RECOVERY, EMPACTA, REMAP-CAP) had in common a high rate of corticosteroid administration, suggesting that the benefit of tocilizumab is specifically in the context of corticosteroid administration.
COVACTA: Tocilizumab in Hospitalized Patients With Severe COVID-19 Pneumonia (Rosas, April 2021).
Overall, in this medium-sized (N=452) Phase 3 randomized controlled trial of hospitalized patients with severe COVID-19 pneumonia who required oxygen, noninvasive ventilation or mechanical ventilation, tocilizumab was associated with a higher median number of ventilator-free days and shorter time to clinical improvement when compared to standard of care but demonstrated no significant difference in clinical status on the ordinal scale. Only 19% of the patients in the tocilizumab arm of the study were also receiving corticosteroids; in other studies where tocilizumab conferred benefit, it was in association with corticosteroids.
Patient population:
- This double-blind randomized, controlled trial examines the use of tocilizumab (8 mg/kg IV) versus placebo (both followed by a second dose within 24 hours if no improvement) among 452 patients with severe COVID-19 pneumonia in nine countries in Europe and North America.
- Eligible patients either had an oxygen saturation of <93% on room air or were receiving supplemental oxygen, or a PaO2/FiO2 ratio of <300 mm Hg.
- The median CRP was 157.2 mg/L (range 1.1-446.6), median IL-6 was 88.1 ng/L (range 3.1-4020) and the median ferritin was 2.3 pmol/mL (range 0-1,657,000).
- At baseline, 38% of patients were receiving mechanical ventilation (23% of them also requiring additional organ support or ECMO, 32% were receiving noninvasive respiratory support, and 26% were receiving supplemental oxygen.
- 294 participants received tocilizumab, and 144 received placebo (2:1 randomization).
- While this study was ongoing (study dates April 3, 2020, to primary completion June 24, 2020), results of the dexamethasone arm of the RECOVERY trial were released (on June 16, 2020), which led to increased use of dexamethasone in patients hospitalized with COVID-19 and requiring oxygen. Therefore, the use of dexamethasone increased in hospitalized patients in the U.S. and the U.K. at the very tail end of this study of tocilizumab, though for most of the study there was limited corticosteroid use.
- More steroids were used in the placebo arm (28.5%) as compared to the tocilizumab arm (19%), which, given the beneficial effects of glucocorticoids, could have biased the results of the study against tocilizumab.
- Mean age was 60.9 years (±14.6). Approximately 45% of participants were over 65 years of age.
- 13% of participants in the tocilizumab group were Black, as compared with 18.1% in the placebo group.
- The median number of days between symptom onset and receipt of drug in the tocilizumab group was 11 days (range 1-49 days).
Primary endpoint:
- Median value for clinical status on seven-category ordinal scale, at 28 days from randomization.
Key findings:
- Patients in the tocilizumab group had a 28-day mortality of 19.7%, as compared to 19.4% in the placebo group. (N.B.: The trial was not powered for the outcome of mortality.)
- Clinical status as measured on an ordinal scale at day 28 was 1.0 in the tocilizumab group and 2.0 in the placebo group (p=0.31).
- Median time to improvement in clinical status was 14 days (95% CI, 12-17) in the tocilizumab arm and 18 days (95% CI, 15-28) in the placebo arm; median time to hospital discharge was 20 days (95% CI, 17-27) in the tocilizumab arm and 28 days (95% CI, 20 days to non-evaluable) in the placebo arm.
- A subgroup analysis among only those participants who also received corticosteroids showed the proportion of participants off oxygen or ready for discharge at day 28 was 41.5% in the tocilizumab arm and 49.4% in the placebo arm.
- Adverse events and severe adverse events occurred at similar rates in the tocilizumab and placebo arms. Serious infection occurred in 21% of tocilizumab recipients, as compared to 25.9% of placebo recipients.
- The mortality rate of patients found in this study is comparable to what has been generally found in hospitalized U.S. COVID-19 patients with inflammatory phase of illness.
Limitations:
- A wide range of inflammatory markers was included (i.e., tocilizumab was not restricted to those with a certain CRP or IL-6 cutoff). Therefore, it is possible that the study population included people who were not experiencing the hyperinflammatory phase of illness that tocilizumab is theorized to decrease.
- Mortality overall was higher in the group of participants who received glucocorticoids than in those who did not, a finding at odds with RECOVERY data on glucocorticoids.
- No pattern of response was seen in patients treated earlier in the course of illness rather than later, a finding at odds with RECOVERY trial data on tocilizumab, which showed slightly better mortality benefit when tocilizumab was given within 7 days of symptom onset than when it was given >7 days from symptom onset.
Interleukin-6 Receptor Antagonists in Critically Ill Patients With COVID-19 (REMAP-CAP Investigators, April 2021).
Overall, in critically ill adult patients with COVID-19 receiving organ support in intensive care, treatment with the IL-6 receptor antagonists tocilizumab and sarilumab improved outcomes, including survival, in this randomized, open-label adaptive platform trial. No increase in serious adverse events was seen in the IL-6 blocker arms as compared to controls. Benefits from IL-6 blockade were seen across all subgroups of CRP in this study of critically ill people with COVID.
Patient population:
- Randomized adaptive platform trial of adult patients with COVID-19 within 24 hours of commencing organ support in an ICU, who were randomized to receive either tocilizumab (8 mg/kg; dose could be repeated if no improvement within 12-24 hours; N=353), sarilumab (400 mg; N=48) or standard of care (control; N=402).
- 29% of the tocilizumab recipients received a second dose of the drug per clinician discretion.
- Glucocorticoids were allowed according to the standard of care in both arms; 93% of participants in this study were on glucocorticoids.
- In the tocilizumab, sarilumab and placebo groups, 74%, 81% and 70% of the patients were men, respectively, and the mean (±SD) age was 61.5±12.5 years, 63.4±13.4 and 61.1±12.8 years, respectively.
- Overall, 4% of the patients were Black, 17% Asian and 72% white, at 113 sites across six countries.
- All but three of the participants were receiving respiratory support, with oxygen through high-flow nasal cannulae (29%), noninvasive ventilation (42%) and invasive mechanical ventilation (29%).
- The majority of enrollments occurred after the June 17, 2020, announcement of the RECOVERY trial data supporting efficacy of dexamethasone; 93% of these received glucocorticoids (and 51% of the 158 participants randomized prior to that point received some form of corticosteroid), and 33% were on remdesivir.
Primary endpoint:
- Respiratory and cardiovascular organ support-free days up to day 21.
- In this composite ordinal outcome, all deaths within hospital are assigned the worst outcome (–1).
- Among survivors, respiratory and cardiovascular organ support-free days are calculated up to day 21, such that a higher number represents faster recovery.
- An odds ratio >1 represented improved survival, more days without organ support or both.
Key findings:
- Median organ support-free days were 10 for tocilizumab (IQR, -1 to 16), 11 for sarilumab (IQR, 0 to 16) and 0 for control (IQR, -1 to 15).
- Relative to control, median adjusted odds ratios for organ support free days were 1.64 (95% credible intervals, 1.25-2.14) for tocilizumab and 1.76 (95% CrI, 1.17-2.91) for sarilumab, yielding >99.9% and 99.5% posterior probabilities of superiority compared with control.
- Hospital mortality was 28% (98/350) for tocilizumab, 22% (10/45) for sarilumab and 36% (142/397) for control.
- Adjusted odds ratio for survival was 1.64 (95% CrI, 1.14-2.35) and 2.01 (95% CrI, 1.18-4.71) in the tocilizumab and sarilumab groups, with 99.6% and 99.5% posterior probability of superiority to control.
- 90-day survival was better in the pooled IL-6 inhibitor groups as compared to control, with a hazard ratio for survival of 1.61 (95% CrI, 1.25-2.08) and >99.9% posterior probability of superiority.
- The estimates of the treatment effect for patients treated either with tocilizumab or sarilumab and corticosteroids in combination were greater than for any intervention on its own.
- Tocilizumab and sarilumab were effective across all secondary outcomes, including 90-day survival, time to ICU and hospital discharge and improvement according to the WHO ordinal scale at day 14.
- There were nine serious adverse events reported in the tocilizumab group, including one secondary bacterial infection, five bleeds, two cardiac events and one deterioration in vision.
- There were 11 serious adverse events in the control group, four bleeds and seven thromboses, and no serious adverse events in the sarilumab group.
Limitations:
- Pragmatic, open-label, adaptive trial design with contemporaneous controls raising the possibility of treatment interactions.
- Outcomes data on 11 participants are missing. Some patients remain hospitalized, so long-term outcomes may differ from the short-term outcomes presented here.
Tocilizumab in Patients Admitted to Hospital With COVID-19 (RECOVERY): Preliminary Results of A Randomized, Controlled, Open-Label, Platform Trial (RECOVERY Collaborative Group, May 2021).
Overall, in this large open-label randomized controlled trial of hospitalized patients with COVID-19 who required oxygen, noninvasive ventilation, or mechanical ventilation and who had evidence of systemic inflammation, tocilizumab reduced 28-day mortality when compared to standard of care; 82% of the patients in the study were also receiving corticosteroids, and the effect of tocilizumab on mortality appeared to be additive to the mortality benefit of corticosteroids.
Patient population:
- This study examined the use of tocilizumab (400-800 mg, weight-based) versus standard of care among 4,116 COVID-19 patients at 131 National Health Service hospitals in the U.K.
- Eligible patients either had an oxygen saturation of <92% on room air or were receiving supplemental oxygen and had a C-reactive protein of ≥75 mg/L.
- The median CRP was 143 mg/dL (IQR, 107-204).
- 14% of patients were receiving invasive mechanical ventilation, 41% were receiving noninvasive respiratory support, and the remaining patients (45%) were receiving supplemental oxygen.
- 2,022 patients were allocated to the tocilizumab arm and 2,094 to the standard of care arm.
- While this study was ongoing, results of the dexamethasone arm of the RECOVERY trial were published, which led to increased use of dexamethasone in patients hospitalized with COVID-19 and requiring oxygen. Therefore, the use of dexamethasone increased in hospitalized patients in the U.K. during this study of tocilizumab.
- 82% of the population was receiving corticosteroids at the time of randomization.
- Mean age was 63.6 years (SD 13.6).
Primary endpoint:
- All-cause mortality within 28 days of randomization.
Key findings:
- The median time between hospitalization and randomization for both groups was 2 days (IQR, 1-5 days).
- The median days since symptom onset in the tocilizumab group was 9 days (IQR, 7-13 days); in the standard of care arm, it was 10 days (IQR, 7-14 days).
- Patients in the tocilizumab group had a lower 28-day mortality (29%) than those in the standard of care group (33%) (RR, 0.86; 95% CI, 0.77-0.96).
- 54% of patients in the tocilizumab group and 47% in the standard of care group were discharged alive within 28 days (RR, 1.22; 95% CI, 1.12-1.34).
- In patients who were not ventilated at baseline, those who received tocilizumab were less likely to be either initiated on mechanical ventilation or die (33% vs. 38%; RR, 0.85; 95% CI, 0.78-0.93).
- In patients receiving corticosteroids, 28-day mortality in the tocilizumab group was 27% versus 33% in the standard of care group (RR, 0.80; 95% CI, 0.70-0.90).
- In patients not on corticosteroids there was no significant difference in mortality (RR, 1.16; 95% CI, 0.91-1.48).
Limitations:
- The mortality rate of patients found in this study is higher than what has been generally found in hospitalized COVID-19 patients in the United States.
- The trial is an open-label design; researchers and patients in the study knew who was receiving which treatment. This could have introduced bias into the results.
- 17% of the patients allocated to the tocilizumab group did not receive the study drug, which may have affected the results.
- Patients without a confirmed SARS-CoV-2 PCR were included; however, in a subgroup analysis of the 94% of patients with PCR-confirmed disease, the results were similar to the overall results.
- Given COVID-19 mortality among hospitalized patients has declined over time, it would be helpful to assess if the mortality difference seen in this study holds when examining only patients from later in the study period.
EMPACTA: Tocilizumab in Patients Hospitalized With COVID-19 Pneumonia (Salama, January 2021).
Overall, in this medium-sized study of hospitalized, nonventilated patients with COVID-19 pneumonia, tocilizumab reduced the likelihood of progression to the composite outcome of mechanical ventilation or death, as compared to placebo, but a mortality benefit was not seen. Notably, this study deliberately set out to include sites with capacity to enroll high-risk and minority patients.
Patient population:
- Hospitalized nonventilated patients with COVID-19 pneumonia were randomized (in a 2:1 ratio) to receive standard care plus one to two doses of either tocilizumab (8 mg/kg IV) or placebo.
- Of the participants overall, 56.0% were Hispanic or Latinx, 14.9% were Black, 12.7% were American Indian or Alaska Native, 12.7% were non-Hispanic white, and 3.7% were of other or unknown race or ethnic group.
Primary endpoint:
- Mechanical ventilation or death by day 28.
- Secondary efficacy outcomes were time to hospital discharge/readiness for discharge using a seven-category ordinal scale for clinical status.
Key findings:
- In the tocilizumab group, the percentage of patients progressing to the primary endpoint of mechanical ventilation or death was 12.0% (95% CI, 8.5-16.9), as compared to 19.3% (95% CI, 13.3-27.4) in the placebo group (hazard ratio for mechanical ventilation or death, 0.56; 95% CI, 0.33-0.97; p=0.04 by the log-rank test).
- Median time to clinical failure was lower in the tocilizumab group, with an HR of clinical failure assessed as a time-to-event analysis of 0.55 (95% CI, 0.33-0.93).
Limitations:
- There was a slight imbalance between receipt of systemic glucocorticoids between the two groups; 80.3% in the tocilizumab group and 87.5% in the placebo group received steroids, which would skew the results away from tocilizumab, as steroids have been shown to decrease mortality in people with severe COVID-19. (Approximately equal numbers, around 79%, received antivirals.)
Efficacy of Tocilizumab in Patients Hospitalized With COVID-19 (Stone, December 2020).
Overall, in this randomized, double-blind, placebo-controlled trial, the use of tocilizumab in patients with elevated inflammatory markers and severe disease did not reduce rates of intubation or death. The findings may be limited by a lack of clarity about where in the disease course patients were randomized.
Study population:
- 243 patients with confirmed COVID-19 (via PCR or IgM), hyperinflammatory states,
- AND at least two of the following signs:
- Fever (body temperature >38°C);
- Pulmonary infiltrates;
- Need for supplemental oxygen in order to maintain an oxygen saturation greater than 92%.
- AND at least one of the following:
- CRP > 50 mg/L;
- Ferritin > 500 ng/mL;
- D-dimer level > 1000 ng/mL;
- LDH > 250 U/L.
- Patients were randomized to receive tocilizumab or placebo in a 2:1 ratio.
- 58% of the population were men, and the median age was 59.8 years (IQR, 21.7-85.4).
- 45% of the sample was Hispanic or Latinx.
- 51% had a BMI of ≥30; 49% of the patients had hypertension, and 31% had diabetes.
Primary endpoint:
- Intubation or death assessed in a time-to-event analysis.
Key findings:
- The HR for intubation or death in the tocilizumab group as compared with the placebo group was 0.83 (95% CI, 0.38-1.81).
- The HR for disease worsening was 1.11 at 14 days (95% CI, 0.59-2.10).
- The median time to discontinuation of supplemental oxygen was 5.0 days in the tocilizumab group and 4.9 days in the placebo group (p=0.69).
- Serious infections occurred less in the tocilizumab group than placebo (8.1% vs. 17.3%; p=0.03).
Limitations:
- Single-center study with relatively small sample size.
- Median time from symptom onset to randomization was not discussed; it is unclear when in the disease course patients received tocilizumab. They may have been ill for a prolonged period of time, or they may have been early in their disease course.
- Patients with a positive IgM were included and may have received tocilizumab later in their course of disease compared to patients who were diagnosed via PCR.
- Patients received other potentially efficacious agents, such as remdesivir and non-dexamethasone glucocorticoids. Eighteen patients in the tocilizumab group and five in the placebo group received steroids.
- The confidence intervals were wide.
Effect of Tocilizumab vs. Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia: A Randomized Clinical Trial (Hermine, October 2020).
Overall, in this small randomized clinical trial of patients with COVID-19 and pneumonia requiring oxygen support but not admitted to the ICU, tocilizumab did not reduce WHO-CPS scores lower than 5 at day 4 but might have reduced the risk of noninvasive ventilation, mechanical ventilation or death by day 14. Results showed no difference in day 28 mortality. The findings may be limited by a lack of clarity around where the patients were in their disease course when randomized.
Study population:
- Patients in nine French hospitals with confirmed SARS-CoV-2 infection with moderate, severe or critical pneumonia.
- Of 130 patients, 63 patients were randomly assigned to the tocilizumab group and 67 to the standard of care group.
- 42 were women (32%), and the median age was 64 years (IQR, 57.1-74.3).
- In the tocilizumab group, antiviral drugs were administered in 11% of patients, glucocorticoids in 33%, and prophylactic or therapeutic anticoagulants in 94%.
- In the standard-of-care group, antiviral drugs were administered in 24% of patients, glucocorticoids in 61%, and preventive or therapeutic anticoagulants in 91%.
Primary endpoint:
- The proportion of patients dead or needing noninvasive or mechanical ventilation on day 4 (score of >5 on the WHO CPS ordinal scale).
- Survival with no need for noninvasive or mechanical ventilation at day 14.
Key findings:
- On day 4, 12 of 63 patients randomized to receive tocilizumab had a WHO-CPS score >5 (19%), compared with 19 of 67 patients in the standard-of-care group (28%) (median posterior absolute risk difference, −9%; 90% CrI, –21 to 3).
- The posterior probability of negative ARD (tocilizumab better than standard of care) was 89.0%, and ARD less than −5.5% was 68.4%.
- On day 14, at least one event (noninvasive ventilation, high-flow oxygen, mechanical ventilation or death) had occurred in 15 patients in the tocilizumab group (24%) (cumulative incidence of event , 24%; 95% CI, 13%-35%) and 24 patients in the standard-of-care group (cumulative incidence, 36%; 95% CI, 33%-58%).
- The posterior probability of any efficacy of tocilizumab (HR<1) was 95.0%, and of moderate or greater efficacy (HR<0.85) was 87.4% (posterior median HR, 0.58; 90% CrI, 0.33-1.00).
- The number of patients with mechanical ventilation or death at day 14 was 11 in the tocilizumab group (17%) and 18 in the standard of care group (27%). The posterior probabilities of HR less than 1 and HR less than 0.85 were 92.5% and 84.4%, respectively (posterior median HR, 0.58; 90% CrI, 0.30-1.09).
- The HR for mechanical ventilation or death was 0.58 (90% CrI, 0.30-1.09).
- At day 28, seven patients had died in the tocilizumab group and eight in the standard of care group (adjusted HR, 0.92; 95% CI, 0.33-2.53).
- Serious adverse events occurred in 20 patients in the tocilizumab group (32%) and 29 in the standard-of-care group (43%) (p=0.21).
Limitations:
- The sample size was small.
- Unblinded study, which could have led to measurement bias.
- There was no placebo.
- Patients may have received antiviral agents, anticoagulants and corticosteroids.
- An analysis of patients with moderate versus severe disease separately was not performed, just ICU vs. non-ICU.
- Includes a narrow segment of the COVID-19 patient population (patients with a WHO-CPS score of exactly 5 and requiring at least 3 L/min oxygen); these results may not be generalizable to other populations.
- The median time from symptom onset to randomization is not discussed; it is thus unclear when the patient received tocilizumab in their disease course. They may have been ill for a prolonged period of time, or they may have been early in their disease course.
- Some harm or benefit could not be ruled out, per authors’ conclusion, as the confidence intervals for efficacy were wide.
Effect of Tocilizumab vs. Standard Care on Clinical Worsening in Patients Hospitalized With COVID-19 Pneumonia: A Randomized Clinical Trial (Salvarani, October 2020).
Overall, in this small randomized clinical trial of hospitalized adult patients with COVID-19 pneumonia and PaO2/FiO2 ratio between 200 and 300 mm Hg who received tocilizumab, there was no observed benefit in disease progression compared with standard of care. The findings may be limited by a lack of clarity around where the patients were in their disease course when randomized.
Study population:
- Prospective, open-label, randomized clinical trial of 126 patients in 24 hospitals in Italy with confirmed COVID-19 pneumonia and PaO2/FiO2 ratio between 200 and 300 mm Hg and either fever or a CRP ≥10 mg/dL and/or CRP level increased to at least twice the admission measurement.
- Patients were excluded if they had advanced age or multiple comorbidities, or if the treating physician deemed the patient wouldn’t receive ICU care.
- 60 patients randomized to tocilizumab; 63 randomized to the control group (intention to treat).
- The median age was 60.0 years (IQR, 53.0-72.0), and 61.1% of patients were male.
- Patients in the control arm had lower C-reactive protein levels, IL-6, ferritin and D-dimer levels and were more frequently treated with antivirals compared with patients in the tocilizumab group at baseline, despite randomization.
Primary endpoint:
- Primary composite outcome including entry into the ICU with invasive mechanical ventilation, death from all causes, or clinical aggravation documented by the finding of a PaO2/FiO2 ratio less than 150 mm Hg, whichever came first.
Key findings:
- 17 of 60 patients in the tocilizumab arm (28.3%) and 17 of 63 patients in the standard-of-care group (27.0%) showed clinical worsening within 14 days after randomization (rate ratio, 1.05; 95% CI, 0.59-1.86).
- 11 patients in total were admitted to ICU, all within 14 days after randomization, with no major differences between the two arms (10.0% vs. 7.9%; rate ratio, 1.26; 95% CI, 0.41-3.91).
- Mortality was comparable at 14 days (1.7% vs. 1.6%; rate ratio, 1.05; 95% CI, 0.07-16.4) and at 30 days (3.3% vs. 1.6%; rate ratio, 2.10; 95% CI, 0.20-22.6) between the two groups.
- The tocilizumab group did not have increased infections compared to the control group.
Limitations:
- Small sample size.
- Lack of a placebo, unblinded study.
- The mortality rate in the study was much lower than the general rate in Italy (2.4% vs. 13.2%).
- Because 14 patients in the control group received tocilizumab after they reached the primary endpoint, subsequent secondary outcomes may have been affected.
- Clinical characteristics differed in the two groups, although they were not statistically significant.
- The median time from symptom onset to randomization is not discussed; it is thus unclear when the patient received tocilizumab in their disease course. They may have been ill for a prolonged period of time, or they may have been early in their disease course. It is also not known what the optimal timing of tocilizumab would be, if it is effective in some situations. A study with variable times to administration would be helpful.
Association Between Early Treatment with Tocilizumab and Mortality Among Critically Ill Patients With COVID-19 (Gupta, October 2020).
Overall, this multicenter retrospective cohort study of critically ill patients with COVID-19 found an association of lower in-hospital mortality risk in patients treated with tocilizumab within the first 2 days of ICU admission, compared with patients whose treatment did not include early use of tocilizumab. However, these findings may be affected by unmeasured confounding.
Study population:
- Retrospective multicenter cohort study of 3,924 adults admitted with COVID-19 to 68 U.S. hospital ICUs from March 4 to May 10, 2020.
- Patients were randomized within the first 2 days of ICU admission.
- The median age was 62 years (IQR, 52-71 years).
- 433 patients received tocilizumab within the first 2 days of ICU admission (11.0%).
- Tocilizumab-treated patients were younger (median age, 58 [IQR, 48-65] years vs. 63 [IQR, 52-72] years) and generally had fewer comorbidities than the non-tocilizumab group:
- Hypertension, 234 (54.0%) vs. 2186 (62.6%).
- Coronary artery disease, 39 (9.0%) vs. 504 (14.4%).
- Congestive heart failure, 23 (5.3%) vs. 386 (11.1%).
- After applying inverse probability weighting, baseline and acute severity-of-illness characteristics were well-balanced between groups.
Primary endpoint:
- Time to death, compared via HRs, and 30-day mortality, compared via risk differences.
Key findings:
- A total of 2,058 patients were discharged alive (52.4%); 1,544 died (39.3%), and 322 remained hospitalized at last follow-up (8.2%).
- The 1,544 patients who died included 125 of the 433 patients treated with tocilizumab (28.9%) and 1,419 of the 3,491 patients not treated with tocilizumab (40.6%) (unadjusted HR, 0.64; 95% CI, 0.54-0.77).
- In the primary analysis, during a median follow-up of 27 (IQR, 14-37) days, patients treated with tocilizumab had a lower risk of death compared with those not treated with tocilizumab (HR, 0.71; 95% CI, 0.56-0.92).
- The estimated 30-day mortality was 27.5% in the tocilizumab-treated patients (95% CI, 21.2%-33.8%) and 37.1% in the non-tocilizumab-treated patients (95% CI, 35.5%-38.7%) (risk difference, 9.6%; 95% CI, 3.1%-16.0%).
Limitations:
- Retrospective study.
- The treatment groups differed at baseline before applying inverse probability weighting, with tocilizumab-treated patients younger and having fewer comorbidities.
- Data collection did not include the number of administered doses of tocilizumab or other administered agents, such as corticosteroids.
- Patients who were hospitalized for 1 week or more before ICU admission were excluded; this could limit the generalizability of the results.
Decreased Mortality in COVID-19 Patients Treated With Tocilizumab: A Rapid Systematic Review and Meta-Analysis of Observational Studies (Malgie, September 2020).
Study population:
- Patients with COVID-19 included in studies that examined tocilizumab use versus no tocilizumab use; studies where tocilizumab was reserved for severe disease or cytokine release syndrome were excluded.
- 10 studies comprising 1,358 patients were included.
- Four studies were from Italy, three were from the U.S., two were from Spain, and one was from France.
Primary endpoint:
- Mortality, expressed as the number of patients who died within the study period.
Key findings:
- Nine of the 10 studies were considered high quality.
- Of the 1,358 patients, 554 patients received tocilizumab, and 804 patients did not.
- There were 95 deaths in the tocilizumab group and 222 deaths in the control group.
- The risk ratio was 0.27 (95% CI, 0.12-0.59); the risk difference was 12% (95% CI, 4.6%-20%) in favor of the tocilizumab group.
- Based on the higher CRP and the lower PaO2-FiO2 ratio for the tocilizumab group, the tocilizumab group appeared to be more severely affected by COVID-19 at baseline than the control group.
- There was substantial heterogeneity with respect to the primary endpoint, with an I2 of 61%; it appeared this was due to one study. When this study was excluded, the I2 was 19%.
- In studies that used glucocorticoids, the treatment effect of tocilizumab on mortality was smaller compared to studies that did not use glucocorticoids (I2=33%).
Limitations:
- The individual studies included in the meta-analysis were observational and thus at risk for bias.
- Multiple confounders exist in the studies included, such as the use of medications for COVID-19, including immunosuppressive medications, differences in the study populations, the dose and timing of tocilizumab, etc.
- The authors used crude risks for the calculation of RR and RD, which does not allow control of baseline imbalances by treatment group.
IL-6 Inhibition in Critically Ill COVID-19 Patients Is Associated With Increased Secondary Infections (Kimmig, October 2020).
Overall, in this small retrospective study of patients with COVID-19, there was a higher incidence of secondary bacterial infections and fungal infections in those that received tocilizumab compared to those not receiving tocilizumab; however, the use of tocilizumab was at the discretion of the primary team, which limits the study findings.
Study population:
- Retrospective study of 111 critically ill COVID-19 patients at a single center in Chicago, of whom 54 received tocilizumab, as per inter-hospital COVID-19 guidance.
- Histopathologic post-mortem findings from several COVID-19 cases that underwent autopsy were also included.
- The mean age in the tocilizumab group was 64.5 years (IQR, 50.9-78.1); 68.5% were male.
- The mean age in the non-tocilizumab group was 61.8 years (IQR, 78.4-45.2); 43.9% were male.
Primary endpoint:
- During an 8-week span, the prevalence of secondary infection and outcomes were compared in patients who did and did not receive tocilizumab.
Key findings:
- Among 54 patients who received tocilizumab, 44 patients (81%) received 400 mg X 1; the rest received doses ranging between 160-800 mg.
- Secondary infections were defined by positive culture data or clinical suspicion resulting in the initiation of antimicrobials.
- Receiving tocilizumab was associated with a higher incidence of secondary bacterial infections, including hospital-acquired pneumonia and ventilator-associated pneumonia (26 [48.1%] vs. 16 [28.1%]; p=0.021).
- Diagnosis of infection was made approximately 5 days after the administration of tocilizumab (4.9±3.0 days; 95% CI, 3.67-6.17).
- Patients who received tocilizumab had higher mortality (35.2% vs. 19.3%; p=0.020).
- Tocilizumab use was independently positively associated with the development of bacterial infections with an odds ratio of 2.76 (95% CI, 1.11-7.20; p=0.0295).
- Seven cases underwent autopsy. In three patients who received tocilizumab, there was evidence of pneumonia on pathology. Of the four patients who had not been given tocilizumab, two showed evidence of aspiration pneumonia, and two exhibited diffuse alveolar damage.
Limitations:
- This is a retrospective study with a lack of randomization; bias is possible.
- The decision to use tocilizumab was at the discretion of the primary team; it is therefore possible there was heterogeneity with determination to use.
- The authors report the higher mortality seen in patients who received tocilizumab was related to secondary infections, but as the use of tocilizumab was not standardized, it is possible patient characteristics not measured in the study made them more likely to receive tocilizumab.
- 19% of the patients who received tocilizumab received non-standard doses (as defined by inter-institutional guidance); the risk for adverse events may have differed by dose.
- The authors note a higher use of immunosuppressive agents in the tocilizumab group (13%) but do not provide further details; the authors note that after removing these patients from the analysis, more patients in the tocilizumab group had bacterial infections, but given the small numbers in the study, it is difficult to interpret this analysis.
Tocilizumab Among Patients With COVID-19 in the Intensive Care Unit: A Multicenter Observational Study (Biran, August 2020).
Overall, in this retrospective cohort study, tocilizumab in patients with severe COVID-19 requiring ICU support was associated with a reduction in hospital related mortality.
Study population:
- Retrospective study of 764 COVID-19 patients admitted to the ICU in 13 New Jersey hospitals; 210 (27%) received tocilizumab.
- Propensity score-matched population included these 210 patients and 420 who did not receive tocilizumab (total of 630 patients).
- Tocilizumab was administered a median of 9 days (IQR, 6-12) after the start of patient-reported symptoms.
Primary endpoint:
- Hospital-related mortality.
Key findings:
- 358 (57%) of 630 patients died; of these, 102 (49%) received tocilizumab and 256 (61%) did not.
- A primary multivariable Cox regression analysis with propensity matching noted an association between receiving tocilizumab and decreased hospital-related mortality (HR, 0.64; p=0.0040).
- In post-hoc analysis of the 558 patients (89%) who had a CRP >15 mg/dL at baseline, tocilizumab exposure was associated with decreased hospital-related mortality (HR, 0.48; p=0.0025). This was not seen in patients with a CRP <15 mg/dL.
- The frequency of secondary bacterial infections was 17% in patients who received tocilizumab and 13% in those who did not.
Limitations:
- This was a retrospective study; while propensity score matching was used, the possibility of confounding still exists.
- No information is given as to how patients were selected to receive tocilizumab, and a convenience sample was used; selection bias is possible.
- Tocilizumab start occurred well after symptoms began (median 9 days).
Tocilizumab in Patients With Severe COVID-19: An Open-Label Retrospective Cohort Study (Guaraldi, August 2020).
Overall, in this retrospective open-label cohort study in patients with severe COVID-19, treatment with tocilizumab was associated with a reduced risk of invasive mechanical ventilation and death; however, secondary infections occurred more often in the tocilizumab group.
Study population:
- 544 hospitalized patients with severe COVID-19, of whom 365 received standard of care and 179 received tocilizumab plus standard of care.
- Standard of care included supplemental oxygen, hydroxychloroquine, azithromycin, antiretrovirals and low molecular weight heparin.
- Patients with severe liver, kidney or hematologic impairments were excluded.
- After baseline, 53 (30%) of 179 patients treated with tocilizumab started glucocorticoids versus 61 (17%) of 365 patients in the standard of care group.
Primary endpoint:
- Composite of mortality or invasive mechanical ventilation.
Key findings:
- 33 (18%) of 179 patients treated with tocilizumab compared to 7 (16%) of 365 patients in the standard of care group needed mechanical ventilation (p=0.41).
- 13 (7%) patients treated with tocilizumab compared to 73 (20%) patients in the standard of care group died (p<0.0001).
- After adjustment for sex, age, recruiting center, duration of symptoms and Sequential Organ Failure Assessment Score, tocilizumab treatment was associated with a reduced risk of invasive mechanical ventilation or death (aHR, 0.61; p=0.020).
- Overall, 24 (13%) of 179 patients treated with tocilizumab were diagnosed with new infections, versus 14 (4%) of 365 patients treated with standard of care alone (p<0.0001).
Limitations:
- As this was a retrospective study, confounding cannot be ruled out.
- Patients also received other therapies for COVID-19.
- The treating physician determined if tocilizumab would be requested for the patient. The study was open label and used a convenience sample.
- Shortages of tocilizumab occurred during the study period. Selection bias is possible.
- The participants who received standard of care only were older and therefore at higher baseline risk of invasive ventilation and death.
Tocilizumab for Treatment of Mechanically Ventilated Patients With COVID-19: A Retrospective Cohort Study (Somers, July 2020).
Overall, in this nonrandomized observational study, tocilizumab use was independently associated with improved survival in patients with severe COVID-19 requiring mechanical ventilation. However, tocilizumab was associated with an increased incidence of secondary infections, primarily bacterial pneumonia.
Study population:
- Retrospective observational, controlled study of 154 patients with severe COVID-19 illness requiring mechanical ventilation at University of Michigan Medical Center.
- 78 patients received tocilizumab (47% treated within 24 hours of intubation; 26% >48 hours of intubation), 76 did not.
- Other therapeutic agents, including hydroxychloroquine, remdesivir and corticosteroids, were also administered.
- Patients who received tocilizumab were younger (mean 55 vs. 60 years), less likely to have chronic pulmonary disease (10% vs. 28%) and had lower D-dimer values at time of intubation (median 2.4 vs. 6.5 mg/dL).
Primary endpoint:
- Survival probability post-intubation.
Key findings:
- In inverse probability of treatment weights-adjusted models, tocilizumab was associated with a 45% reduction in hazard of death (HR, 0.55; 95% CI, 0.33-0.90).
- Tocilizumab was associated with improvement on a six-point ordinal scale that incorporated mechanical ventilation, development of superinfection and discharge from the hospital (OR, 0.6; p≤0.03 for inverse probability of treatment-weighted (IPTW) models).
- Patients who received tocilizumab were more than twice as likely to develop a superinfection compared to untreated controls (54% vs. 26%; p<0.001), driven primarily by a large increase in ventilator-associated pneumonia (45% vs. 20%; p<0.001).
Limitations:
- As this was a retrospective study, confounding cannot be ruled out.
- The treating physician determined if tocilizumab would be requested for the patient; selection bias is possible.
- A concurrent trial of sarilumab occurred at the institution during the study period. Patients who were ineligible for that trial were eligible for this study, which may limit the generalizability of the results.
- Patients treated with tocilizumab also received other therapeutic agents.
- Baseline differences in the study populations may have confounded the results.
Additional Literature
Observational Study on Off-Label Use of Tocilizumab in Patients With Severe COVID-19 (Albertini, September 2020). In this single-center observational cohort study of 44 patients hospitalized with COVID-19, 22 patients diagnosed with COVID-19 were treated with tocilizumab and were compared with 22 patients not treated with tocilizumab. The average respiratory rate was lower in the tocilizumab group than in the control group (21.5 vs. 25.5 breaths/min at day 14; 95% CI, −7.5 to −0.4; p=0.03). Patients tended to be intubated less during the course of the disease (2/22 vs. 6/22; 95% CI, −0.4 to 0.1; p=0.12).
Tocilizumab Treatment for Cytokine Release Syndrome in Hospitalized COVID-19 Patients: Survival and Clinical Outcomes (Price, June 2020). In this retrospective observational study of 239 hospitalized patients with COVID-19, 104 (44%) of whom had severe COVID-19, in 153 patients who received tocilizumab, 14-day survival was 87% and did not differ according to disease severity (83% vs. 91%; p=0.11).
Impact of Low Dose Tocilizumab on Mortality Rate in Patients With COVID-19 Related Pneumonia (Capra, June 2020). In this retrospective observational study of 85 hospitalized patients in Italy with COVID-19 with respiratory failure not requiring mechanical ventilation, 62 received tocilizumab; these patients showed a significantly greater survival rate as compared to standard of care (hydroxychloroquine, lopinavir and ritonavir; hazard ratio for death, 0.035; p=0.004), adjusting for baseline clinical characteristics.
Back to Top
Anti-GM-CSF Antibodies
The cytokine GM-CSF is 10-fold higher in people who died from COVID-19 than people with mild COVID. Because it is upstream in the cascade of cytokine release, it was theorized that blocking GM-CSF would provide more benefit in blocking a hyperinflammatory response to SARS-CoV-2 infection than blocking individual cytokines, such as IL-6. Emerging data also suggests that GM-CSF may play a more prominent role in propagating the immune response to COVID-19 in older individuals (>70 years) than in younger individuals, which establishes a foundation for a potentially differential effect of the anti-GM-CSF agents by age, with greater benefit for older age groups (Thwaites, October 2020 – preprint, not peer-reviewed).
Based on this, a monoclonal antibody targeting GM-CSF, lenzilumab (Humanigen), was tested under emergency FDA Investigational New Drug application in a small cohort of patients (N=12) who were hospitalized with severe COVID-19 pneumonia, and its outcomes were compared to the outcomes of a matched control cohort (Temesgen, November 2020). The study found that time to clinical improvement was significantly shorter for the lenzilumab-treated group compared with the untreated cohort, with a median of 5 days versus 11 days (p=0.006). There was also a significant difference in the oxygenation status, as measured by change in SpO2/FiO2 ratio from baseline (day 0) through day 14 post-therapy, between the two groups (ANOVA, p<0.001), and in the percentage of patients with acute respiratory distress syndrome (defined as SpO2/FiO2 <315 mm Hg) (ANOVA, p<0.001). The follow-on LIVE-AIR Phase 3 trial showed highly promising results and is described in detail below. Also currently recruiting is the NIH-supported ACTIV-5 study, a Big Effect Trial, which is a proof-of-concept study designed to identify promising candidate treatments to enter into a later, more definitive study. The BET-B stage will evaluate the combination of remdesivir with lenzilumab versus remdesivir with a lenzilumab placebo.
Another monoclonal antibody binding the GM-CSF receptor, mavrilimumab, was associated with earlier oxygenation improvement and shorter hospitalization in a small cohort of hospitalized patients (De Luca, June 2020). The following extremely small MASH-COVID trial (N=40 enrolled out of an originally planned N of 60) was a randomized, placebo-controlled trial, which was stopped early due to slow enrollments and showed no benefit from mavrilimumab, but called for larger studies to be done (Cremer, March 2021). In parallel, otilimab, another anti-GM-CSF agent currently in Phase 3 studies for rheumatoid arthritis, was studied in a Phase 2 study (OSCAR study) in patients with severe COVID-related pulmonary disease. It missed meeting its primary endpoint of significant clinical improvement, but showed a significant benefit in a subgroup of 180 older patients (>70), with respect to both respiratory improvement and death; currently, the study is enrolling 350 more older patients, with results forthcoming. Lenzilumab has received FDA approval for compassionate use in the COVID-19 setting. Other anti-GM-CSF monoclonal antibodies, TJ003234, namilumab and regimsilumab/gimsilumab, are also being studied, with prospective randomized controlled studies ongoing which will provide more information on possible clinical benefit from these agents.
Guidelines
IDSA and NIH guidelines have not yet been released for anti-GM-CSF antibodies.
Key Literature
Lenzilumab Efficacy and Safety in Newly Hospitalized COVID-19 Subjects: Results From the LIVE-AIR Phase 3 Randomized Double-Blind Placebo-Controlled Trial (Temesgen, May 2021 - preprint, not peer-reviewed).
Overall, this large randomized, placebo-controlled trial demonstrated that participants with severe COVID-19 who received the intravenous anti-GM-CSF monoclonal antibody lenzilumab had a higher likelihood of survival without ventilation than participants given placebo, and that this was especially true in people with CRP levels <150 mg/L and age <85 years.
Patient population:
- Adult participants (N=520) with COVID-19 who had ≤94% oxygen saturation on room air but were not yet requiring invasive mechanical ventilation were randomized to receive 600 mg of IV lenzilumab (N=261) or placebo (N=259).
- Lenzilumab was administered as three infusions given 8 hours apart.
- Participants were 64.7% male, with a mean (SD) age of 60.5 years and mean BMI 32.5 kg/m2; 8% self-reported as minorities.
- Study took place at 29 sites in the U.S. (85% of participants) and Brazil (15% of participants).
- Mean CRP level was 98.36 mg/L; 77.9% of participants had CRP <150 mg/L.
- At baseline, 40.5% were on high-flow oxygen or noninvasive positive pressure ventilation , and 59.5% were on low-flow supplemental oxygen or had SpO2 <94% on room air.
- Comorbidities included obesity (55.1%), diabetes (53.4%), chronic kidney disease (14.0%) and coronary artery disease (13.6%).
- Subjects also got corticosteroids (93.7%), remdesivir (72.4%) or both (69.1%).
Primary endpoint:
- Composite endpoint of ventilator-free survival (also called survival without ventilation), at day 28.
- Failure to meet the primary endpoint was defined as death or the need for invasive mechanical ventilation.
- Key secondary endpoints: proportion of IMV, ECMO or death, mortality and time to recovery (measured with eight-point clinical status scale).
Key findings:
- Participants randomized to the lenzilumab group had greater likelihood than those on placebo of meeting the primary endpoint of SWOV (mITT HR, 1.54; 95% CI, 1.02-2.31, p=0.041; ITT HR, 1.90; 95% CI, 1.02-3.52; nominal p=0.043).
- Separation of Kaplan-Meier survival curves began around day 3, and the separation continued to increase over 28 days.
- SWOV significantly better (i.e., there was an even greater impact on survival) in the following subgroups:
- Participants who got both corticosteroids and remdesivir (ITT, 1.92; 95% CI, 0.20-3.07; nominal p=0.0067);
- Participants with CRP <150 mg/L and age <85 years (mITT HR, 2.96; 95% CI, 1.63-5.37; nominal p=0.0003 and second sensitivity analysis on ITT group showing survival improved 2.23-fold with nominal p=0.003);
- Participants hospitalized ≤2 days prior to randomization (HR, 1.88; 95% CI, 0.13-3.12; nominal p=0.015).
- When looked at alone and not as part of a composite endpoint with ventilation need, mortality was significantly improved by 2.17-fold in subjects with CRP <150 mg/L and age <85 years (nominal p=0.040).
- Both time to recovery and incidence of IMV/ECMO or death were not significantly different between the study groups EXCEPT among participants with CRP <150 mg/L and age <85 years (36% improved with nominal p of 0.012, and OR 0.32 [95% CI, 0.15-0.65; nominal p=0.002], respectively).
- Lenzilumab decreased CRP levels over the time period from day 2 to day 28 but only in subjects with a baseline CRP <150 mg/L.
- Sigmoidal relationship between CRP and benefit from lenzilumab.
- Adverse events ≥ Grade 3 were observed in 26.7% and 32.7% of the lenzilumab and placebo recipients, respectively; severe adverse events were similar across the groups.
Limitations:
- A few of the sites in Brazil experienced a large surge in COVID cases during the study, with corresponding limited access to basic supportive COVID-19 care, resulting in the need to escalate directly to invasive mechanical ventilation because of the lack of devices for noninvasive provision of low-flow oxygen. (These sites were excluded while the study was still blinded, however.)
- There was significant non-prespecified subgroup analysis in this paper, which can be problematic as it is vulnerable to bias.
- Composite, surrogate outcomes can be problematic, and thresholds for intubation were likely heterogenous across institutions.
Back to Top
JAK Inhibitors
Artificial intelligence algorithms have predicted several candidate drugs among FDA-approved agents that have particularly high potential to be repurposed as potent therapies for COVID-19 and its associated lethal cytokine storm (Richardson, February 2020). One such candidate is baricitinib, an orally administered, selective Janus kinase 1 and JAK2 inhibitor currently FDA-approved for the treatment of rheumatoid arthritis, which is being evaluated in multiple studies for treatment of COVID-19. The hypothesized mechanism of its benefit relates both to its potent antiviral activity and to dampening cytokine signaling, which contributes to inflammation. The drug has an inhibitory effect on proteins in the host cell membrane — AP2-associated protein kinase 1 and cyclin G-associated kinase, which are key in regulating receptor-mediated endocytosis of many viruses, including SARS-CoV-2 (Jorgensen, July 2020).
Two randomized controlled trials — the) and COV-BARRIER study—have evaluated the use of baricitinib (4 mg daily for 14 days or until discharge) in patients hospitalized with COVID-19. In the large (N=1033) ACTT-2 study, hospitalized (non-ICU) participants were randomized to receive combination therapy with baricitinib and remdesivir (intervention) or remdesivir alone (control) (Kalil, March 2021). The duration of symptoms prior to receipt of study product was > 7 days in 83.3% and less than 7 days in only 16.7%. Most participants did not receive dexamethasone, as the study was largely conducted before the results of the RECOVERY trial showing mortality benefit from dexamethasone. Participants who received the combination of baricitinib and remdesivir had a shorter median time to recovery of 7 days (95% CI, 6-8), as compared with 8 days (95% CI, 7-9) in the control group (rate ratio for recovery, 1.16; 95% CI, 1.01-1.32; p=0.03), and a 30% higher odds of improvement in clinical status at day 15 (OR, 1.3; 95% CI, 1.0 -1.6) The baricitinib group had similar rates of progression of respiratory disease or death as compared to participants on remdesivir alone (27.8% vs. 30.5%; OR, 0.85 (95% CI, 0.67-1.08). They also had a nonsignificant difference in day 28 mortality (5.1% vs. 7.8%; rate ratio: 0.65; 95% CI, 0.39-1.09) and were somewhat less likely to require initiation of mechanical ventilation or ECMO through day 29 (10% vs. 15.2%; RR, 0.66; 95% CI, 0.46-0.93). The greatest benefit from baricitinib was seen in participants requiring supplemental oxygen or noninvasive ventilation at baseline, with unclear benefit in participants who were already mechanically ventilated at baseline.
The even larger (N=1,525) COV-BARRIER randomized controlled phase 3 study examined treatment of hospitalized patients with severe COVID-19 with baricitinib plus standard of care as compared to standard of care alone (note that in this trial, the standard of care given to participants included corticosteroids in 79% and antivirals in 18.9%) (Marconi, May 2021 - preprint, not peer-reviewed). The study did show, for its secondary endpoint, a 28-day mortality benefit with baricitinib compared to placebo (HR, 0.57; 95% CI, 0.41-0.78), but no statistically significant difference between arms in the composite endpoint (progression to needing high-flow oxygen, noninvasive and invasive mechanical ventilation [OR, 0.85; 95% CI, 0.67-1.08]). While it would be desirable to be able to show some discrete mechanism to explain the mortality benefit, the fact that a mortality benefit was demonstrated despite similar rates of discrete insults such as thrombotic and cardiovascular events between arms may speak to the multidimensional, multiorgan mechanism of mortality from severe COVID-19, which is, as the world is now painfully aware, protean in its devastation.
Another JAK inhibitor, tofacitinib, which selectively inhibits JAK1 and JAK3 with functional selective inhibition of JAK2, resulting in blockage of intracellular transduction once a cytokine has bound to its receptor and decreased interferon and IL-6 production by helper T cells, has been studied in patients hospitalized with COVID-19. In the STOP-COVID trial, at 15 sites in Brazil, 289 hospitalized participants with COVID-19 pneumonia not yet requiring mechanical ventilation were randomized to receive either tofacitinib 5 to 10 mg administered orally twice daily or placebo for 14 days or until discharge from the hospital (Guimarães, July 2021). A composite primary outcome of death or the need for mechanical ventilation (assessed on an ordinal scale with eight categories) was assessed at day 28 from study entry. Overall, 89.3% of the patients also received glucocorticoids during hospitalization — 88.9% in the tofacitinib group and 89.7% in the placebo group (for dexamethasone alone, 68.8% and 76.6% received it in the tofacitinib and placebo groups, respectively). The results showed a lower incidence of death or respiratory failure in the tofacitinib group as compared to the placebo group (18.1% and 29%, respectively (RR, 0.63; 95% CI, 0.41-0.97; p=0.04). A sensitivity analysis adjusted for glucocorticoid use showed a similar outcome. There was a nonsignificant trend toward better scores on the ordinal scale with tofacitinib as compared with placebo, at both day 14 and day 28 (proportional odds of 0.60 [95% CI, 0.36-1.00] at day 14 and 0.54 [95% CI, 0.27-1.06] at day 28). Of particular note, the benefit of tofacitinib held true in sensitivity analyses regardless of the duration of symptoms prior to tofacitinib receipt, including in patients with >10 days of symptoms prior to receipt of drug, who had more benefit from tofacitinib than patients with 0-10 days of symptoms prior to tofacitinib receipt. This cuts against the conventional wisdom that earliest possible treatment will confer maximal benefit (which may well be true for antivirals), and instead points to a potential rolling benefit of sequential addition of JAK inhibitors over time, perhaps after the initiation of steroids, in patients vulnerable to cytokine cascade (which may be the more fitting model for immunomodulators).
Safety
Overall, while baricitinib can increase risk of thrombosis and other adverse events in clinical trials of individuals taking it over a long period of time for rheumatoid arthritis, the shorter duration used for COVID treatment appears generally safe and well tolerated; adverse events and severe adverse events reported with the use of baricitinib for COVID are similar to those in the control arms. In the ACTT-2 study, participants were recommended to receive prophylaxis against venous thromboembolism, and in that context the percentage with venous thromboembolism was similar across the two treatment groups (21 patients [4.1%] vs. 16 patients [3.1%]; absolute difference 1%, 95% CI, -1.3 to 3.3) (Kalil, March 2021). Patients receiving baricitinib and remdesivir had a lower risk of developing serious adverse events through day 28 (16% vs. 21%; RR, 0.76; 95% CI, 0.59-0.99), and there were fewer new infections noted in the baricitinib plus remdesivir group compared with remdesivir group alone (30 patients [5.9%] vs. 57 patients [11.2%]). However, among the participants who received glucocorticoids, there were more infections than in those who did not (25.1% and 5.5%, respectively; it is unclear how many of each of those groups also received baricitinib). In the STOP-COVID tofacitinib trial, safety was reassuring: adverse events occurred in 26.1% of the patients in the tofacitinib group and in 22.5% of those in the placebo group, and serious adverse events were observed in 14.1% in the tofacitinib group and in 12.0% in the placebo group (Guimarães, July 2021). The incidence of serious secondary infections was 3.5% in the tofacitinib group and 4.2% in the placebo group. There was a slightly higher incidence of adverse events leading to permanent discontinuation of the study drug in the tofacitinib arm (11.3%, as compared to 3.5% in the placebo arm, and most of those were elevated aminotransferase levels and lymphopenia).
It is still somewhat unclear whether baricitinib or tofacitinib plus remdesivir will give as much benefit as dexamethasone alone, as head-to-head comparisons are lacking. Preliminarily, some investigators have shown a survival benefit from the addition of tofacitinib to dexamethasone (over dexamethasone alone) in a cohort of largely African American hospitalized patients in the Mississippi Delta (adjusted odds ratio for death: 0.30; 95% CI, 0.12-0.76; p=0.01, after adjusting for age and clinical parameters) (Hayek, June 2021). Further long-term data, especially around 60-day mortality, will be forthcoming from the COV-BARRIER study. Also, while it is reasonable to assume that immunomodulators will have the greatest impact if given early in the course of disease, there was an extended duration of symptoms prior to receipt of drug in both the ACTT-2 and COV-BARRIER studies. (In an important counterpoint, the tofacitinib STOP-COVID trial showed greater benefit from JAK blockade in participants with a longer duration of symptoms than among those with a shorter duration of symptoms.) Also needed are trials comparing in a head-to-head manner baricitinib (or tofacitinib) + tocilizumab or looking at the combination compared to tocilizumab alone.
Guidelines
IDSA guidelines suggest baricitinib rather than no baricitinib for hospitalized adults with severe COVID-19 (SpO2 ≤94% on room air, or requiring supplemental oxygen, oxygen through a high-flow device or noninvasive ventilation) but not yet requiring mechanical ventilation (conditional recommendation, moderate certainty of evidence).
IDSA guidelines also endorse using baricitinib with remdesivir rather than remdesivir alone, for hospitalized patients with severe COVID-19 not yet requiring mechanical ventilation, who for whatever reason cannot receive corticosteroids (conditional recommendation, low certainty of evidence). Recommended baricitinib dosing is a 4 mg daily dose for 14 days or until hospital discharge.
FDA revised in December of 2021 its EUA for baricitinib for the treatment of COVID-19 in hospitalized patients 2 years of age or older who require supplemental oxygen, mechanical ventilation (either noninvasive or invasive) or ECMO.
The recommended dosage of baricitinib under the EUA is:
- Adults and pediatric patients 9 years of age and older: 4 mg once daily.
- Pediatric patients 2 years to less than 9 years of age: 2 mg once daily.
- Duration is for 14 days or until hospital discharge, whichever comes first.
- Renal dose adjustments are recommended, listed in the FDA EUA factsheet, Table 1.
Key Literature
STOP-COVID: Tofacitinib in Patients Hospitalized With COVID-19 Pneumonia (Guimarães, July 2021).
Patient population:
- Adult participants (N=289) hospitalized with COVID-19 pneumonia but not yet requiring invasive mechanical ventilation were randomized to receive 5-10 mg of oral tofacitinib twice daily for up to 14 days or placebo.
- Participants were 34.9% female, with a mean (SD) age of 56 ± 14 years; 4% were white.
- Study took place at 15 sites in Brazil.
- Overall, 89.3% of the patients also received glucocorticoids during hospitalization: 9% in the tofacitinib group and 89.7% in the placebo group (for dexamethasone alone, 68.8% and 76.6% received it in the tofacitinib and placebo groups, respectively).
Primary endpoint:
- Composite endpoint of death or the need for mechanical ventilation (assessed on an ordinal scale with eight categories) at day 28.
Key findings:
- There was a lower incidence of death or respiratory failure in the tofacitinib group as compared to the placebo group (18.1% and 29%, respectively [RR, 0.63; 95% CI, 0.41-0.97; p=0.04).
- A sensitivity analysis adjusted for glucocorticoid use showed a similar outcome.
- There was a nonsignificant trend toward better scores on the ordinal scale with tofacitinib as compared with placebo, at both day 14 and day 28 (proportional odds of 0.60 [95% CI, 0.36-1.00] at day 14 and 0.54 [95% CI, 0.27-1.06] at day 28).
- Benefit of tofacitinib held true in sensitivity analyses in patients with >10 days of symptoms prior to receipt of drug, who had more benefit from tofacitinib than patients with 0-10 days of symptoms prior to tofacitinib receipt.
- Adverse events occurred in 26.1% of the patients in the tofacitinib group and in 22.5% of those in the placebo group.
- Serious adverse events were observed in 14.1% in the tofacitinib group and in 12.0% in the placebo group.
- Incidence of serious secondary infections was 3.5% in the tofacitinib group and 4.2% in the placebo group.
- There was a slightly higher incidence of adverse events leading to permanent discontinuation of the study drug in the tofacitinib arm (11.3%, as compared to 3.5% in the placebo arm, and most of those were elevated aminotransferase levels and lymphopenia).
Limitations:
- No remdesivir was available in Brazil at the time of the study, so an ACTT-2-comparable analysis of JAK inhibitor with or without remdesivir could not be performed (it is however a strength of this study that it looked at JAK inhibitor with steroids compared to steroids alone).
- Differential proportions of dexamethasone use between the two groups, which is known to confer survival benefit.
- Not powered to detect a mortality benefit.
COV-BARRIER: Efficacy and Safety of Baricitinib in Patients With COVID-19 Infection: Results From the Randomized, Double-Blind, Placebo-Controlled, Parallel-Group COV-BARRIER Phase 3 Trial (Marconi, May 2021 - preprint, not peer-reviewed).
Patient population:
- Adult participants (N=1,525) hospitalized with COVID-19 were randomized to receive 4 mg of once daily oral baricitinib twice daily for up to 14 days or placebo.
- The mean age of the participants was 57.6 years (SD 14.1); 63.1% (N=963) were male.
- 6% (920/1,493) of participants were white, 11.7% (174/1493) were Asian, and 5.0% (75/1,493) were Black/African American.
- The majority (83.3% [1,265/1,518]) of participants had symptoms ≥7 days prior to enrollment.
- Clinical status at baseline was OS 4 for 12.3% (186/1,518), OS 5 for 63.4% (962/1,518) and OS 6 for 24.4% (370/1,518) of participants.
- Overall, standard-of-care treatment included systemic corticosteroids in 79.3% [1,204/1,518] of participants.
- 3% (1,099/1,204) received dexamethasone.
- 189% (287/1,518) of participants received remdesivir.
- Study took place at 101 sites in 12 countries in Asia, Europe, and North and South America.
- Percentages of enrollments: Brazil (22,1%, N=337), United States (21%, N=320), Mexico (184%, N=281) and Argentina (13.6%, N=208).
- Baseline median CRP value was 65.0 mg/L (67.5 mg/L for baricitinib group and 62.0 mg/L for placebo group).
- Median duration of symptoms prior to receiving study product was 8.5 days.
Primary endpoint:
- Composite endpoint of progression to high-flow oxygen, noninvasive ventilation or invasive mechanical ventilation or death by day 28.
- Key secondary endpoint: all-cause mortality by day 28.
- Key exploratory endpoint: all-cause mortality by day 60.
Key findings:
- Overall, there was no significant difference in meeting the primary endpoint (27.8% of baricitinib group vs. 30.5% of the placebo group progressed to death or the need for ventilatory support [OR, 0.85; 95% CI, 0.67-1.08; p=0.18).
- However, the secondary endpoint of 28-day all-cause mortality occurred in 8.1% (N=62) for baricitinib as compared to 13.1% (N=100) for placebo, corresponding to a 38.2% reduction in mortality in the baricitinib group (HR, 0.57; 95% CI, 0.41-0.78; nominal p=0.0018).
- Number needed to treat to prevent one additional death of 20.
- The exploratory endpoint of 60-day all-cause mortality was observed in 10.3% (N=79) for baricitinib and 15.2% (N=116) for placebo (HR, 0.62; 95% CI, 0.47-0.83; p=0.0050).
- A significant reduction in mortality was observed for participants with baseline severity subgroup Ordinal Scale 6 with baricitinib compared with placebo (17.5% [32/183] vs. 29.4% [55/187]; HR, 0.52, 95% CI, 0.33-0.80; nominal p=0·0065), corresponding to a number needed to treat to prevent one death of 9.
- Incidence of serious adverse events was similar in the two groups (14.7% [N=110] vs. 18.0% [N=135] in the baricitinib and placebo groups, respectively).
- Incidence of serious infections was also similar (8.5% [N=64] vs. 9.8% [N=74]) in baricitinib and placebo groups.
- Incidence of venous thromboembolic events was also similar across groups (2.7% [n=20] in the baricitinib group vs. 2.5% [n=19] in the placebo group).
Limitations:
- No control for multiple comparisons.
- Day 28 mortality was a secondary endpoint, with nominal p-value reported.
- Pronounced evolution in the standard of care over the course of the trial.
- Primary outcome based on ordinal scale reflects decisions of treating physicians, which could be based on heterogeneous and cultural factors across sites.